49 year old patient with vomitings
This is an a online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
CASE:
A 49-year-old male auto driver by occupation resident of lingottam case to the casualty with chief complaints of vomiting and decreased appetite since 2 days.
History of presenting illness:
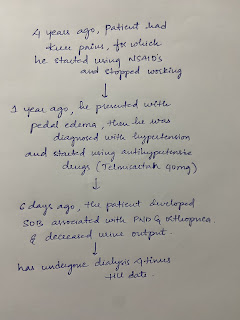
Patient was apparently asymptomatic 10 years back then he developed fever and generalized weakness for which he went to a local hospital. There he was diagnosed with diabetes to which he was started on metformin. Later after 1 year he developed headache to which he consulted a doctor and was diagnosed with Hypertension to which he used medication for 1 year and stopped using medication. Then 6 years back he developed weakness of limbs for which he was diagnosed to have low potassium and treated conservatively. Then 20 days back he developed headache and vomitings 10 times in a day to which he consulted a local RMP where he was administered glucose. Then he developed right sided paralysis to which he was referred to a higher centre where he was diagnosed with acute ischaemic stroke later he was discharged and sent home. Later he had 2 such hospitalizations in the past 20 days. Then 3 days back he woke up at night and started having vomitings 10 to 15 times a day non bilious, non projectile to which he went to local hospital and then admited here.
Daily Routine:
He wakes up at 5 30 am goes to drive auto has breakfast around 8 continues with his work later has lunch around 1 pm continues his work till 8pm in between he has tea in the evening. Reches home at 8 has dinner and goes to bed by 9 30 pm.
There was no change in his daily routine when he was diagnosed with diabetes. But he was unable to go to work since the past 20 days
Past History:
K/c/o Diabetes since 10 years (on metformin 500mg)
K/c/o Hypertension since 6 years used medication for 1 year and stopped
History of acute ischaemic stroke 20 days back
No history of CAD, TB, EPILEPSY and ASTHMA
Personal History:
Diet: Mixed
Appetite: Decreased
Sleep: Disturbed
Bladder movements: Regular
Bowel movements: Irregular
He drinks alcohol 2 to 3 times a week from past 15 years
He smokes 10 cigarettes every day from past 25 years
Family History: Not significant
General Examination:
The patient was conscious, coherent, and cooperative.
Well-oriented to time, place, and person.
Pallor- absent
Icterus- absent
Cyanosis absent
Clubbing- absent
Geheneralized lymphadenopathy-absent
Bilateral pedal edema- absent





Vitals:
Temperature- 98.8 F
Pulse rate- 76 bpm
Blood pressure- 140/90 mm Hg
Respiratory rate- 20 cpm
Spo2-98%
GRBS- 205mg/dl
Systemic Examination:
Cardiovascular system: S1, S2 heard no murmurs heard
Respiratory system: Normal vesicular sounds heard, bilateral air entry present.
Abdomen: Soft and nontender, no hepatomegaly, spleen not palpable.
Central Nervous System: No focal neurological deficits
INVESTIGATIONS:
Ultrasound:



Provisional Diagnosis:
Diabetic ketoacidosis because of poor glycemic control with acute ischemic stroke.
Treatment:
IVF NS 0.9%
Inj HAI 5 units
Inj Zofer 4mg
Inj PAN 40mg
T. Ecosprin 75mg
T. Atorva 20mg
T. Clopitab 75mg
Syrup Sucralfate 10ml
T. Pregabel M 75mg


Comments
Post a Comment